Best CBD Oil for Pain Relief & Inflammation: Highest Quality Brands On The Market

Over the past three years, CBD oil has become increasingly popular as a health and wellness supplement.
One of the main reasons people are interested in trying CBD oil is because of its pain-killing benefits. We’ll get into the details of how CBD is suggested to help with pain later, along with some suggestions for the best CBD oils for pain and inflammation.
The ability for CBD to help with pain is a significant advantage over conventional pain management options — which often involve addictive and potentially harmful medications. Instead, this natural supplement has very few side effects and an exceptional safety profile — all without compromising on effectiveness.
At A Glance: Our Top 3 Picks for CBD Oil for Pain Relief & Inflammation
This is an important question to ask because the truth of the matter is that not all CBD oils work. Many simply contain too little CBD to be of any help, while others contain harmful contaminants like heavy metals, pesticides, or chemical solvents — all of which could add to the pain you’re already experiencing by damaging the sensitive nerve cells around the body.
We’re going to cover all of this in the article below. You’ll learn how to spot a high-quality CBD oil and how current evidence shows CBD to work inside the body.
This is a big topic, so let’s get started with our list of top-rated CBD oils for pain.
| IMAGE | PRODUCT | |
|---|---|---|
| Best Overall  | Royal CBD
| CHECK BEST PRICE → |
| Best Organic  | Gold Bee
| CHECK BEST PRICE → |
| Runner Up  | CBDPure
| CHECK BEST PRICE → |
Top 10 Best CBD Oil Brands for Pain Management in 2023
Not sure which CBD oil to buy to help with chronic pain? Before we get into the nitty-gritty of how CBD is suggested to work for pain and inflammation, here’s our top 5 list of CBD oils I’ve used myself for back pain.
We’ll also offer some advice on a few ways you can spot a trustworthy CBD vendor even if they didn’t quite make it onto our list.
I’ve been using CBD for over 5 years now and I’ve stumbled upon some stellar companies with top-notch oils and fly-by-night businesses with oils that can’t simply don’t work.
I have a relatively short list of CBD brands that I fully trust and I want to share my choices with you so you can avoid some of the headaches and disappointment I’ve already endured.
Here are my top 10 CBD oil brands for pain:
1. Royal CBD (Best CBD Oil On The Market)
Technical Details
| Total CBD Content | 250 – 2500 mg |
| Available Flavors | Natural, Mint, Vanilla, Berry |
| Potency | 8.3 – 83.3 mg/mL |
Get 15% off all Royal CBD products. Use code “CFAH” at checkout.
Why Royal CBD is My Top Pick:
As skeptical as I am towards the majority of new CBD brands, I decided to give Royal CBD a try because I liked the company’s dedication to quality. I love seeing companies that take what they do seriously.
You can tell right away from the color, flavor, and consistency of the oil that you’re dealing with a product well above average.
This oil is cheaper than most of the other premium CBD oils I’ve tried, comes in a full range of potencies, and uses some of the best full-spectrum hemp extracts I’ve ever seen. I’ve heard friends using this brand for quite some time and decided to give it a try for myself — so I ordered a few bottles in different strengths.
After taking the Royal CBD’s 2500mg full-spectrum CBD oil for just over a week, I noticed an improvement in my back pain. There was a time when I had serious problems falling asleep because of the sharp pains in my back that seemed to intensify whenever I laid down to fall asleep. It was a nightmare. I’d lay awake for hours changing positions to try and find a spot that didn’t leave me writhing in discomfort.
With this oil, my experience went far beyond what I expected. Not only did it help ease the pain, but my overall quality of sleep improved. I mean, I didn’t sleep longer but I began to wake up rested and with a clear head.
My favorite combination for this particular oil is the vanilla in the 1000 mg bottle. This is the largest potency option currently offered by Royal CBD and has the best value overall. I took the oil twice per day, once in the morning when I woke up, and again in the evening before bed. One bottle of the 1000 mg CBD oil lasted me about a month.
Pros |
Cons |
|
|
2. Gold Bee (Best Organic CBD Oil)
Pros |
Cons |
|
|
What I Like About Gold Bee:
I honestly believe Gold Bee makes the best organic CBD products out there. The brand combines premium Colorado-grown hemp with organic honey sourced from the Brazillian Rainforest. While Gold Bee offers a modest selection of oils — with up to 1200 mg of CBD per bottle — the formula is spot-on when it comes to the quality of ingredients. I’m totally not going to complain about the potency, as my back pain and sleep quality got better than with some high-strength oils I’ve tried in the past. Considering the quality of these products, they actually come at a bargain price. If you want to try other formats from Gold Bee, you can choose between its high-strength capsules and CBD-infused honey.
3. CBDPure (Runner Up)

Technical Details
| Total CBD Content | 100 – 600 mg |
| Available Flavors | None |
| Potency | 1.6 – 10 mg/mL |
What I Like About CBDPure CBD Oil:
I love how transparent this company is. If I were judging companies solely by their transparency level, CBDPure would have scored the second place, right after Royal CBD. The company provides all the details about each stage of production when making this CBD oil. You can find all the third-party lab test results for each batch on the product page — something we’ve come to expect from any high-quality CBD company.
What really makes this company stand out is its incredible satisfaction guarantee. If you order the product and decide it wasn’t working for you, simply send it back and get a full refund. This satisfaction guarantee extends over 3 whole months — which is about three times longer than the industry average.
I keep a bottle or two of CBDPure oil in my medicine cabinet for achy moments after a run or hike with the kids.
The only real downside to this oil is the potency — which comes in denominations of 1.5, 5, and 10 mg/mL. This is suitable for more minor symptoms, but may not be enough for people with heavy CBD demands.
Pros |
Cons |
|
|
4. HempBombs

Technical Details
| Total CBD Content | 300 – 4000 mg |
| Available Flavors | Unflavored, Acai Berry, Orange Creamsicle, Peppermint, Watermelon |
| Potency | 10 – 133.3 mg/mL |
What I Like About HempBombs:
I used HempBombs CBD isolate-based hemp oil for quite some time before switching to full-spectrum CBD oil and in my opinion, this is the best brand when it comes to CBD isolates. Their products contain 99% pure CBD and ZERO THC.
Now don’t get me wrong, CBD isolates are great, they offer consistent doses of CBD, contain 0% THC, and are generally cheaper than their full-spectrum counterparts. In most cases, I like using a full-spectrum extract like Royal CBD oil because of something called the entourage effect — which is a concept highlighting the phenomenon where cannabinoids like CBD tend to work better when other hemp-derived compounds are also present.
In isolates, the only cannabinoid present is CBD.
HempBombs CBD oil is available in five different strengths — from 300mg to 4000mg per bottle. The CBD is added in the form of a 99% pure isolate — which means there’s going to be virtually no traceable amounts of any other cannabinoids, including THC, CBC, CBG, or CBN.
You can also buy these oils in different flavors. Hemp Bombs often adds new flavors to the list, but my all-time personal favorite is the Acai berry. It’s not too sweet but adds a really pleasant flavor to the otherwise bland CBD and MCT oil formula.
Pros |
Cons |
|
|
5. CBDistillery

Technical Details
| Total CBD Content | 250 – 5000 mg |
| Available Flavors | None |
| Potency | 8.3 – 166 mg/mL |
What I Like About CBDistillery:
CBDistillery is now one of the largest CBD companies in North America. The company began in 2016 as a legacy brand for Balanced Health Botanicals.
Over the years, CBDistillery has had the chance to really dial-in its CBD oil formula. The company now sells its CBD oil in two formats — “full-spectrum” and “THC-free.” The THC-free option is great for people who want to benefit from the synergy of CBD and other cannabinoids but without bringing any THC whatsoever into their system.
Even the full-spectrum option contains less than 0.3% THC — which is well below the amount needed to cause any psychoactive effects. These oils are both completely non-psychoactive.
You can choose between five different strengths, starting at 250mg up to 5000mg of CBD per bottle. This covers just about every range of potencies you would ever need. We recommend opting for the higher potency options because they have the best value overall. The higher potency you purchase, the further your dollar gets you.
The more potent options also las the longest because you need smaller amounts of the oil each time to get the desired dose of CBD.
I tried the 1000mg bottle to keep myself calm during the first few months after giving birth to my first son and I must admit it helped me maintain my sanity during that time. I found it to have a remarkable calming effect on the body and mind.
Pros |
Cons |
|
|
6. NuLeaf Naturals

Technical Details
| Total CBD Content | 240 – 4850 mg |
| Available Flavors | None |
| Potency | 48.5 mg/mL |
What I Like About NuLeaf Naturals
Nuleaf Naturals is one of the most popular CBD companies in the United States — most likely related to how long the company has been in the business of selling CBD. Nuleaf naturals were one of the first CBD companies to enter the mainstream market.
Despite the companies longstanding reputation, Nuleaf Naturals only sells one CBD oil. When you go to the website you’ll find a few different options, including a pet oil — but it’s important to understand that these are all the exact same full-spectrum extract, the only difference is the bottle sizes.
We love the simplicity of Nuleaf Naturals product lineup. The oils come with a decent potency of around 48 mg/mL, and just about every bottle size you can imagine. This makes it easy for everybody to find a product that works for them regardless of the budget.
With that said, if you have the cash, we highly recommend getting the larger bottle sizes in order to get the best value for your money.
You can choose between five different sizes:
- 5mL — 240mg of CBD
- 15mL — 725mg of CBD
- 30mL — 1450mg of CBD
- 50mL — 2425mg of CBD
- 100mL — 4850mg of CBD
Pros |
Cons |
|
|
7. Charlotte’s Web

Technical Details
| Total CBD Content | 200 – 1800 mg |
| Available Flavors | Mint Chocolate, Lemon Twist, Orange Blossom, Olive Oil |
| Potency | 7 – 60 mg/mL |
About Charlotte’s Web:
Charlotte’s Web is one of the pioneers in the American CBD industry. Established by the Stanley Brothers, the company has coined a reputation of a trustworthy manufacturer by helping now late Charlotte Figi with her treatment-resistant epilepsy. Although the company has recently received a warning letter from the FDA due to their health claims, they still have many faithful customers and a massive number of positive reviews on the web.
Charlotte’s Web CBD oil comes in several potencies: 200 mg, 500 mg, 1500 mg, and 1800 mg of CBD per bottle. The highest strength offers 60 mg of full-spectrum CBD per milliliter. There are two bottle sizes to choose from: 30 mL and 100 mL; Charlotte’s Web also has flavored variants of its CBD oil, including Lemon Twist, Orange Blossom, Mint Chocolate, and Olive Oil.
What could the company do better?
First off, they could change their extraction method because they use ethanol, which is less efficient than CO2 extraction. Secondly, and most importantly, the suspension in olive oil makes them taste a bit bitter — even in the flavored versions.
Pros:
- One of the most reputable brands on the market
- Full-spectrum CBD
- Delicious flavored versions
- Up to 1800 mg of CBD per bottle
- Available in two sizes: 30 mL and 100 mL
- Third-party tested for potency and purity
Cons:
- Non-organic hemp
- Ethanol extraction
- Suspension in olive oil (bitter taste)
- The company received a warning letter from the FDA in the past due to inappropriate health claims
8. cbdMD

Technical Details
| Total CBD Content | 300 – 7500 mg |
| Available Flavors | Natural, Berry, Orange, Mint |
| Potency | 10 – 250 mg/mL |
About cbdMD:
cbdMD is another popular manufacturer that offers a wide range of CBD extracts, from tinctures to gummies to capsules, bath bombs, topicals, sleep aids, and pet products.
The brand offers a wide range of pure CBD oils, with up to 7500 mg of CBD per bottle. The highest potency comes with a whopping dose of 200 mg of pure CBD suspended in MCT oil for higher bioavailability and a smoother flavor. cbdMD also has three flavored CBD oils: Berry, Orange, and Mint.
Despite an impressive potency range, cbdMD uses broad-spectrum CBD in their products, which doesn’t evoke the full entourage effect. The higher potency may not necessarily mean better results in this case.
The company has high transparency standards; not only does cbdMD broadly describe their activity from farming to testing, but they also provide batch-specific certificates of analysis for their products, including the results for potency and common contaminants like pesticides, heavy metals, and residual solvents.
Pros:
- US-grown, non-GMO hemp
- CO2 extraction
- THC-free
- Up to 7500 mg of CBD per bottle
- Batch-specific certificates of analysis
Cons:
- Limited entourage effect due to the lack of THC
- Most people don’t need such high doses of CBD in their routine
9. Medterra

Technical Details
| Total CBD Content | 500 – 3000 mg |
| Available Flavors | Natural, Citrus, Mint Chocolate |
| Potency | 16 – 100 mg/mL |
About Medterra:
Medterra is a small craft company from California. The brand offers premium CBD oils in different spectra: full-spectrum CBD, broad-spectrum CBD, and isolates. The potency of these products ranges between 500 mg and 3000 mg of CBD per bottle, which is a standard range. On top of the unflavored version, there are two flavored options: Citrus and Chocolate
Medterra prides itself on making the real full-spectrum CBD because each bottle of its full-spectrum CBD oil comes with 2 mg of THC. However, these products are only legal in the states that have legalized higher amounts of THC for recreational use. So, if you want to buy the company’s products in all 50 states, your options are limited to broad-spectrum CBD and CBD isolate. These provide more CBD per bottle — upwards of 1000 mg.
The entire Medterra’s product range is tested in a third-party laboratory for their CBD content and safety.
Pros:
- Premium-grade CBD oils
- Up to 3000 mg of CBD per bottle
- Available as full-spectrum CBD, broad-spectrum CBD, and isolates
- Lab tested for potency and purity
Cons:
- The “real” full-spectrum CBD oil isn’t available in all states
- Some of the lab reports indicate higher CBD levels than stated on the bottle
- No discounts for returning customers
10. Joy Organics

Technical Details
| Total CBD Content | 450 – 900 mg |
| Available Flavors | Tranquil Mint, Fresh Lime, Summer Lemon |
| Potency | 15 – 30 mg/mL |
About Joy Organics:
Joy Organics holds the reputation of one of the most reputable CBD vendors in the industry. The company was established by a woman named Joy Smith, who has been using CBD oil to manage her problems with pain and sleep. After experiencing the benefits of CBD first-hand, she has decided to share her passion for cannabis with other health-conscious consumers.
The brand sells a range of broad-spectrum CBD products from certified organic hemp. They have many positive reviews all over the Internet; they also haven’t received any warning letter regarding health claims from the FDA — unlike many companies in this space (even the veterans like Charlotte’s Web).
The Joy Organics CBD oil features a broad-spectrum CBD formula in a modest potency range, from 450 to 900 mg of CBD per bottle. You can choose from three refreshing flavors: Summer Lemon, Fresh Lime, and Tranquil Mint. The strongest version of the Joy Organics CBD oil contains 30 mg of broad-spectrum CBD in every milliliter, which is a standard dose for most people who take CBD oil for daily supplementation.
In 2018, one of the company’s flavored CBD oils was found to contain a fungicide that is commonly sprayed on citrus fruit during independent lab testing. Fortunately, Joy Organics recalled the product shortly after this incident and implemented a new third-party testing system to make sure there are no flaws in the end product.
Pros:
- Non-GMO, US-grown hemp
- Supercritical CO2 extraction
- Broad-spectrum CBD
- THC-free
- Delicious flavors
Cons:
- A bit expensive
- No high-strength oils
CBD Oil for Pain Management: Complete Guide for Beginners

Now that we’ve covered a few CBD oil options that are going to provide the best value for your money, let’s discuss how CBD is suggested to support chronic pain in the first place. We’ll also cover some of the most common ways people are using CBD oil for pain.
What is CBD Oil?
CBD stands for cannabidiol _ it’s one of the primary active ingredients in the cannabis plant. It’s completely non-psychoactive and offers a wide range of benefits to the human body.
CBD oil is a combination of a CBD extract, with a carrier oil to help dissolve and store the CBD. Most CBD oils use carrier oils like MCT oil, or hemp seed oil — which is then combined with CBD isolate, or full-spectrum hemp extract rich in CBD and other similar cannabinoids.
Cannabinoids like CBD are fat-soluble — which means they dissolve when mixed with oil, but won’t dissolve in water. By dissolving these compounds in an oil solution, the CBD becomes much easier to store and use. Instead of measuring out micrograms of CBD crystals or hemp resin, all you need to do is measure oil to get your dose of CBD. This can be done using a simple dropper that comes standard with most CBD oils.
Because of their ease of use, and long shelf-life, CBD oils have become the go-to method of using CBD and other hemp extracts.
You can also opt-out to use CBD-infused gummies if you wanted something discreetly, read our in-depth review on CBD Gummies to understand better.
How Does CBD Work?
Cannabis has been used for managing pain and inflammation for thousands of years.
The earliest records of the medical use of the herb date back to ancient China when the emperor Shen-Nung placed it among other therapeutic substances in the Chinese pharmacopeia (1). The leaves were wrapped around an injury as a poultice to reduce pain and discomfort, and reverse swelling and bruising.
Despite being a known medicine for a long time, scientists have only recently begun to unlock the mechanisms cannabis uses to achieve its important pain-killing benefits.
Since the discovery of the endocannabinoid system in 1992, CBD and other phytocannabinoids have been in the spotlight of modern medicine.
The endocannabinoid system is one of the most important neurochemical networks in the human body (2). It works by interacting with the endocannabinoid system — a series of hormones and receptors that help regulate over a dozen core processes in the human body. The active compounds in the cannabis plant are very similar to the naturally-produced hormones involved with our endocannabinoid system.
By interacting with the endocannabinoid system, CBD and other cannabinoids are able to modulate several key processes, such as:
- Appetite
- Immune function
- Memory
- Mood
- Stress
- Sensory perception (including pain)
- Inflammation
- Reproductive health
- Nerve function
- Sleep
How Can CBD Reduce Pain Transmission?
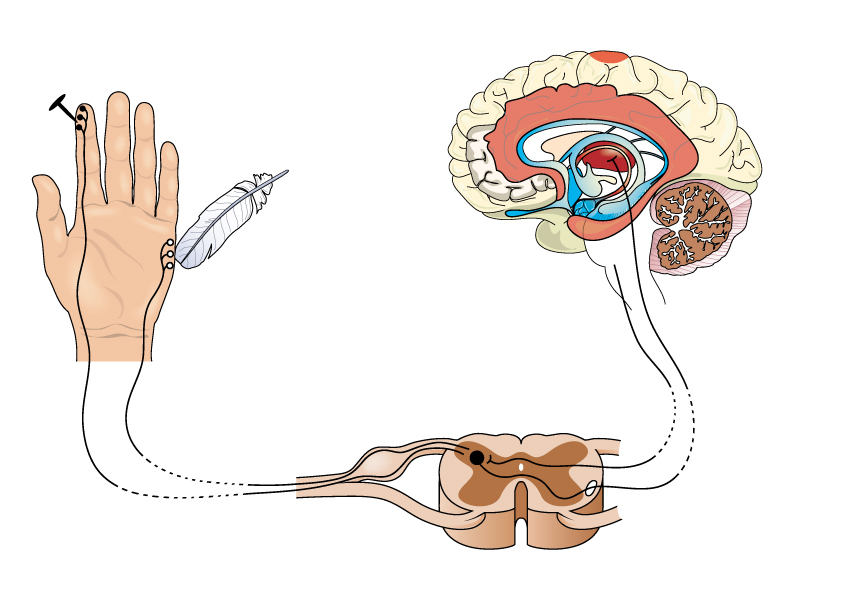
How does all of this relate to pain? The answer lies in the way pain is transmitted to the brain.
When we injure ourselves, cells in the immediate vicinity begin releasing compounds that trigger a cascade of inflammation and sensory activation — which is what triggers the pain transmission.
The pain signal is then sent to the spinal cord through a network of nerves distributed all around the body.
Once in the spine, the pain signal is sent through a gateway (opioid and vanilloid receptors) designed to limit the amount of signal that ends up in the brain for processing. This works like a border crossing. The border security decides whether or not you’re allowed to enter and what you can take with you.
In the context of pain, these gateways can limit the amount of pain signal that continues across the border to the brain. If more pain signal is allowed to pass, the brain perceives more pain. If the pain is stopped at the border, the brain perceives less pain.
Conventional pain medications work by activating the opioid receptors acting as a key gateway for pain transmission to the brain.
Related: Best Natural Pain Relievers
CBD has a similar effect, but through a different receptor is known as the vanilloid receptors. These vanilloid receptors are tasked with regulating a specific form of pain caused by either heat or inflammation. CBD has been reported to modulate this vanilloid receptor — leading to a reduction in the pain signals sent to the brain from inflammatory causes such as arthritis, muscle damage, or infection, to name a few.
CBD has other ways it can limit pain transmission as well:
- CBD may reduce inflammation, limiting the initial cause of pain in the body
- CBD acts as an antioxidant, helping the body resist and recover from damage
- CBD relaxes muscle fibers, reducing pain caused by muscle spasms and tightness
More research is needed to fully understand how CBD and other active cannabinoids can block pain. Every year dozens of new research papers are published in an attempt to paint a clear picture of how CBD works, how to get the most benefit from the supplement, and what its limitations are.
Choosing CBD Oil Companies: How to Differentiate the Good From the Bad
CBD has become a lucrative business. Companies are selling a myriad of different CBD oils and other products in an attempt to cash in on the new health trend. This means there are a lot of excellent products coming to market, but it also means there’s a lot of trash as well. It’s important as a CBD user that you understand what makes a CBD oil good, and what makes it bad so you can avoid wasting your money, or worse — using CBD oils that contain harmful or damaging ingredients.
Let’s cover the most important points to remember when looking for CBD oil online retailers.
1. Check the Hemp Source
The source of the hemp used to make the oil is vitally important when it comes to determining which CBD oils are the best. The main reason comes down to the botany of the hemp plant itself.
Hemp is a bio-accumulator — which means it has the tendency to absorb compounds from the soil and accumulate them in its leaves, stems, and roots. The deep taproots of the hemp plant stretch far beneath the soil, pulling out and storing all the heavy metals and other elements it can find in the soil.
This aspect is in part why hemp is so nutritious, but it also means that plants grown in contaminated soils often contain contaminants that can be harmful to your health. Some of the worst offenders are heavy metals — which can build up in the body over time and lead to severe long-term health effects.
You want to avoid consuming heavy metals at all costs.
Poorly grown hemp could contain heavy metals, as well as other contaminants like mycotoxins, or pesticide residues that will end up in the CBD oil after all the processing is complete.
For this reason, it’s important to purchase CBD oil from companies that account for this effect. Only buy from company’s that make an effort to source hemp from organic farms, and take measures to assess every batch of hemp that enters the facility to determine heavy metal, microbial contaminant, and pesticide contamination.
The best hemp sources tend to come from states like Oregon, Colorado, or Alabama, as well as neighboring countries like Canada or Scandinavian countries. These places are all known for having high standards for hemp cultivation, and clean soils.
2. Look for CO2 Extracted Products
Once the company has the hemp, they need to extract the CBD from it. You can do this in many different ways using solvents like ethanol, methanol, hexane, ether, or butane. All of these solvents work to strip the active compounds from the hemp plant and can then be evaporated to leave behind a pure CBD-rich resin.
however, there’s a problem with these solvents.
Even in professional lab settings, it can be very difficult to remove all traces of these solvents from the final product. Most of these solvents are toxic to the human body, even in trace amounts.
Therefore, the best companies are using another method to strop the active ingredients from the starting hemp material. This method uses CO2 placed under high pressure. the high pressure and temperature control convert the CO2 into a phase that’s neither liquid nor gas. This special state is referred to as being supercritical.
Supercritical CO2 acts just like any other solvent, but with one key benefit — as soon as the pressure is relieved, the gas evaporates completely, leaving behind no harmful chemical residues.
when shopping for CBD oil, it’s ideal to look for a company that uses supercritical CO2 to extract the CBD rather than the toxic solvents mentioned above. Supercritical CO2 is very expensive and highly technical — but usually produces a far superior product in the end.
If a company is using harsh solvents like butane or propane (or they don’t tell you anything about their extraction methods), it’s a sign that you should look for another brand.
3. Ask for Third-Party Lab Reports
Every company has the option to send their products to an independent lab or third-party testing.
These laboratory tests check for the entire cannabinoid profile of the extract and are able to detect over 200 common contaminants.
Before a CBD product becomes available for sale, it should pass the laboratory test for potency and purity. If any inconsistencies are shown between different batches of the same product, the company should rework it and send it for analysis once again.
High-quality CBD companies will continually send each batch of product to a lab with no affiliation to the company (called a third-party or independent lab) for testing. These results are then published publicly on the website for customers to view.
The best companies will take this even one step further — adding a database and batch numbers on every bottle of CBD oil so you can view the results for your specific bottle of oil. Third-party testing is now an industry standard.
Always buy your CBD oil from companies that show third-party lab reports on their website. Only then will you know what’s inside the bottle before you even order a product. If the company is producing CBD oil that’s as high quality, as they say, there should be nothing to hide in these lab tests and they should be listed publicly on the company website. If you can’t find them on the site, you can ask customer service for these as well.
If these tests don’t exist, or you can’t track them down from the website or customer service — it’s best to avoid this company and move on to another that takes this important step seriously.

What the Research Says About Using CBD Oil for Pain:
Understanding how CBD works is no simple task. This compound is incredibly complex — working through a number of unrelated receptors around the body, interacting with enzymes, cell membranes, and various other cell structures. This makes studying CBD very difficult.
Nevertheless, there have been thousands of research papers published on medical marijuana — seeking to understand the interaction between cannabinoids like CBD and the human body. A lot of this research specifically focused on the effects of CBD on various forms and causes of pain. Let’s explore some of the results this research has yielded in the context of pain management.
1. CBD Oil for Chronic Back & Nerve Pain
The painkilling properties of cannabidiol have been most thoroughly studied in animal models, as well as a handful of human clinical trials.
One of the best studies we have available on the topic is a meta-analysis published in 2017. This analysis looked at 24 different clinical trials involving 1,334 patients over several years and demographics. These studies all used various forms of cannabis for treating chronic pain. The analysis reports that many of these studies showed a reduction in chronic pain scores by 50% or more (3) — suggesting the cannabis plant to be a potential treatment for chronic pain.
Another clinical trial looked at the effects of a combination of CBD to THC in the treatment of intractable cancer pain. This study found that twice as many people in the treatment group given CBD and THC had a 30% or more reduction in pain symptoms at the conclusion of the trial (6).
Even though more clinical trials on humans are needed to gauge how CBD affects specific forms of pain or other conditions, scientists believe the efficacy of CBD in treating chronic pain is related to its anti-inflammatory effects (3).
2. CBD Oil for Arthritis
CBD has had a lot of research as a potential alternative to prescription and non-prescription pain medications commonly used for alleviating arthritis pain.
Researchers have found a clear link between the endocannabinoid system and the pathophysiology of osteoarthritis, which is a degenerative joint disease associated with chronic pain and inflammation (4).
One of the key areas CBD is thought to support osteoarthritis specifically is through the effects on an enzyme known as 5-lipoxygenase — AKA 5-LOX. CBD has been shown to inhibit this enzyme (7), which converts fatty acids into pro-inflammatory compounds. These inflammatory messengers have been shown to be a key component in the underlying inflammation involved with osteoarthritis (8).
By reducing the underlying causes of arthritis pain, CBD is thought to reduce the overall burden of pain from the condition over the long term.
3. CBD and Multiple Sclerosis (MS) Pain
Due to its antioxidant and anti-inflammatory properties, CBD is a potent neuroprotective — which is how experts believe CBD is able to relieve debilitating MS pain, —which affects roughly 50–70% of patients diagnosed with the condition.
A study conducted on animals at Cajan Institute tested the anti-inflammatory effects of CBD on mice the researchers wanted to find out if CBD can provide a reversed inflammatory response on those cells. After ten days, the researchers found a reduction in inflammatory markers with a rodent encephalitis model designed to imitate the impact MS has on the body (5).
More research is needed to see exactly how these effects are translated to humans. Currently, there are 23 clinical trials currently underway, or planned within the next 12 months seeking to explore the effects of CBD on MS.
4. CBD Oil in Sports: Injuries & Muscle Endurance
Cannabidiol can be applied in two different ways when it comes to pain and physical activities. For example, when you administer CBD orally in the form of oil as a post-workout, it helps alleviate the muscle inflammation that troubles athletes once they go beyond the edge again.
If, however, you’re suffering from an injury, it’s best to apply CBD topically. Its anti-inflammatory and neuroprotective properties allow the cannabinoid to relieve pain and improve regeneration capacities.
Does CBD Have Any Side Effects?

The main reason why parents are so enthusiastic about CBD is that this cannabinoid is completely non-intoxicating, doesn’t cause addiction, and has only a few mild side effects when taken at excessive doses.
Research shows that even doses up to one and a half grams have no severe side effects on human health (9).
Despite being a notoriously safe supplement, there are some side effects of using CBD in high doses. Let’s cover the most common side effects people report from using CBD:
- Anxiety
- Brain fog
- Reduced appetite
- Mood changes
- Diarrhea or constipation
- Dizziness or lightheadedness
- Drowsiness or fatigue
- Dry mouth
- Nausea and vomiting
The most common side effect by far, like other forms of cannabis, is dry mouth. This is best managed by taking your CBD oil along with some juice like pineapple or orange juice.
Another common side effect is lowered blood pressure, which may trigger another unwanted reaction — lightheadedness. This side effect is important to consider if you suffer from low blood pressure already or are taking blood pressure-lowering medications.
Always consult your doctor before using CBD or other cannabis extracts if you’re taking prescription medications or have underlying medical conditions.
In Summary: Buying CBD Oil For Pain
As CBD becomes more popular around the world, scientists are publishing new research on cannabinoids on a near-weekly basis. As time goes on, experts are mapping out the complicated mechanisms CBD and other hemp derivatives are using to support both acute and chronic pain of all different origins.
Here are the main takeaways from the current research:
- CBD inhibits inflammation at several different levels
- CBD offers antioxidant support
- CBD may relieve muscle tension and inflammation
- CBD interacts with the vanilloid receptors in the brain responsible for regulating inflammatory pain transmission
When it comes to pain, CBD appears to target the cause of the problem instead of just masking its symptoms.
Getting relief on so many levels and without any harmful side effects or risk of addiction is the reason why CBD oil has become so popular over the past half a decade.
I hope this guide has managed to clear up any confusion regarding CBD oil and pain, and given you the insight necessary to find the right CBD oil for the job.
Have you tried CBD oil for chronic pain? Did you feel any difference? Let me know in the comments below!
References:
- Brand, E. J., & Zhao, Z. (2017). Cannabis in Chinese Medicine: Are Some Traditional Indications Referenced in Ancient Literature Related to Cannabinoids?. Frontiers in pharmacology, 8, 108.
- Alger B. E. (2013). Getting high on the endocannabinoid system. Cerebrum: the Dana forum on brain science, 2013, 14.
- Aviram, J., Samuelly-Leichtag, G. (2017) Efficacy of Cannabis-Based Medicines for Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Physician, 20(6), E755-E796.
- Bruni, N., Della Pepa, C., Oliaro-Bosso, S., Pessione, E., Gastaldi, D., & Dosio, F. (2018). Cannabinoid Delivery Systems for Pain and Inflammation Treatment. Molecules (Basel, Switzerland), 23(10), 2478.
- Elliott, D. M., Singh, N., Nagarkatti, M., & Nagarkatti, P. S. (2018). Cannabidiol Attenuates Experimental Autoimmune Encephalomyelitis Model of Multiple Sclerosis Through Induction of Myeloid-Derived Suppressor Cells. Frontiers in immunology, 9, 1782.
- Johnson, J. R., Burnell-Nugent, M., Lossignol, D., Ganae-Motan, E. D., Potts, R., & Fallon, M. T. (2010). Multicenter, double-blind, randomized, placebo-controlled, parallel-group study of the efficacy, safety, and tolerability of THC: CBD extract and THC extract in patients with intractable cancer-related pain. Journal of pain and symptom management, 39(2), 167-179.
- Takeda, S., Usami, N., Yamamoto, I., & Watanabe, K. (2009). Cannabidiol-2′, 6′-dimethyl ether, a cannabidiol derivative, is a highly potent and selective 15-lipoxygenase inhibitor. Drug Metabolism and Disposition.
- Lascelles, B. D. X., King, S., Roe, S., Marcellin‐Little, D. J., & Jones, S. (2009). Expression and activity of COX‐1 and 2 and 5‐LOX in joint tissues from dogs with naturally occurring coxofemoral joint osteoarthritis. Journal of orthopaedic research, 27(9), 1204-1208.Chicago